Decreased lung function after preschool wheezing rhinovirus illnesses in children at risk to develop asthma
Abstract
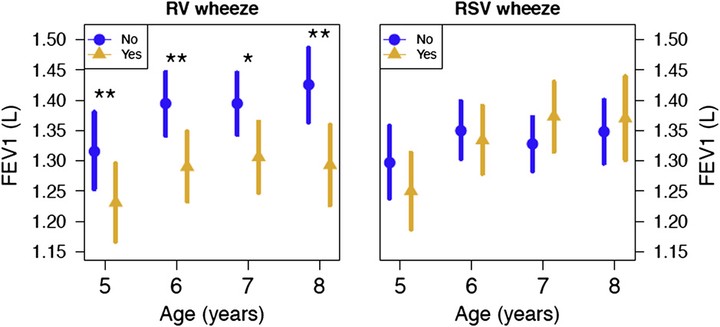
BACKGROUND: Preschool rhinovirus (RV) wheezing illnesses predict an increased risk of childhood asthma; however, it is not clear how specific viral illnesses in early life relate to lung function later on in childhood. OBJECTIVE: To determine the relationship of virus-specific wheezing illnesses and lung function in a longitudinal cohort of children at risk for asthma. METHODS: Two hundred thirty-eight children were followed prospectively from birth to 8 years of age. Early life viral wheezing respiratory illnesses were assessed by using standard techniques, and lung function was assessed annually by using spirometry and impulse oscillometry. The relationships of these virus-specific wheezing illnesses and lung function were assessed by using mixed-effect linear regression. RESULTS: Children with RV wheezing illness demonstrated significantly decreased spirometry values, FEV(1) (P = .001), FEV(0.5) (P < .001), FEF(25-75) (P < .001), and also had abnormal impulse oscillometry measures–more negative reactance at 5 Hz (P < .001)–compared with those who did not wheeze with RV. Children who wheezed with respiratory syncytial virus or other viral illnesses did not have any significant differences in spirometric or impulse oscillometry indices when compared with children who did not. Children diagnosed with asthma at ages 6 or 8 years had significantly decreased FEF(25-75) (P = .05) compared with children without asthma. CONCLUSION: Among outpatient viral wheezing illnesses in early childhood, those caused by RV infections are the most significant predictors of decreased lung function up to age 8 years in a high-risk birth cohort. Whether low lung function is a cause and/or effect of RV wheezing illnesses is yet to be determined.